




Deep Plane Facelift - Explanation
The original form of facelift as a deep plane facelift was originally described by Dr. Sam Hamra (Dallas/Tx, USA) in 1990 as a composite facelift. The term “deep plane” = “deep layer” is defined by the surgical technique of loosening the tissue in a deep layer and leaving the superficial layers intact (i.e. in the composite). This achieves particularly natural results and a long-lasting facelift. A “tightened” or even “over-tightened” appearance is avoided. The most modern form, the so-called extended deep plane facelift, represents a consistent further development based on intensive anatomical research and was popularized by Dr. Bryan Mendelson (Melbourne/Australia) and Dr. Andrew Jacono (New York/NY, USA). In its current methodology, the technique has only reached its highest and most effective stage of development in the last five years or so and is only performed by very few surgeons. It is usually combined with a neck lift in order to achieve particularly harmonious results. The advantages of a deep plane facelift are explained in more detail below.
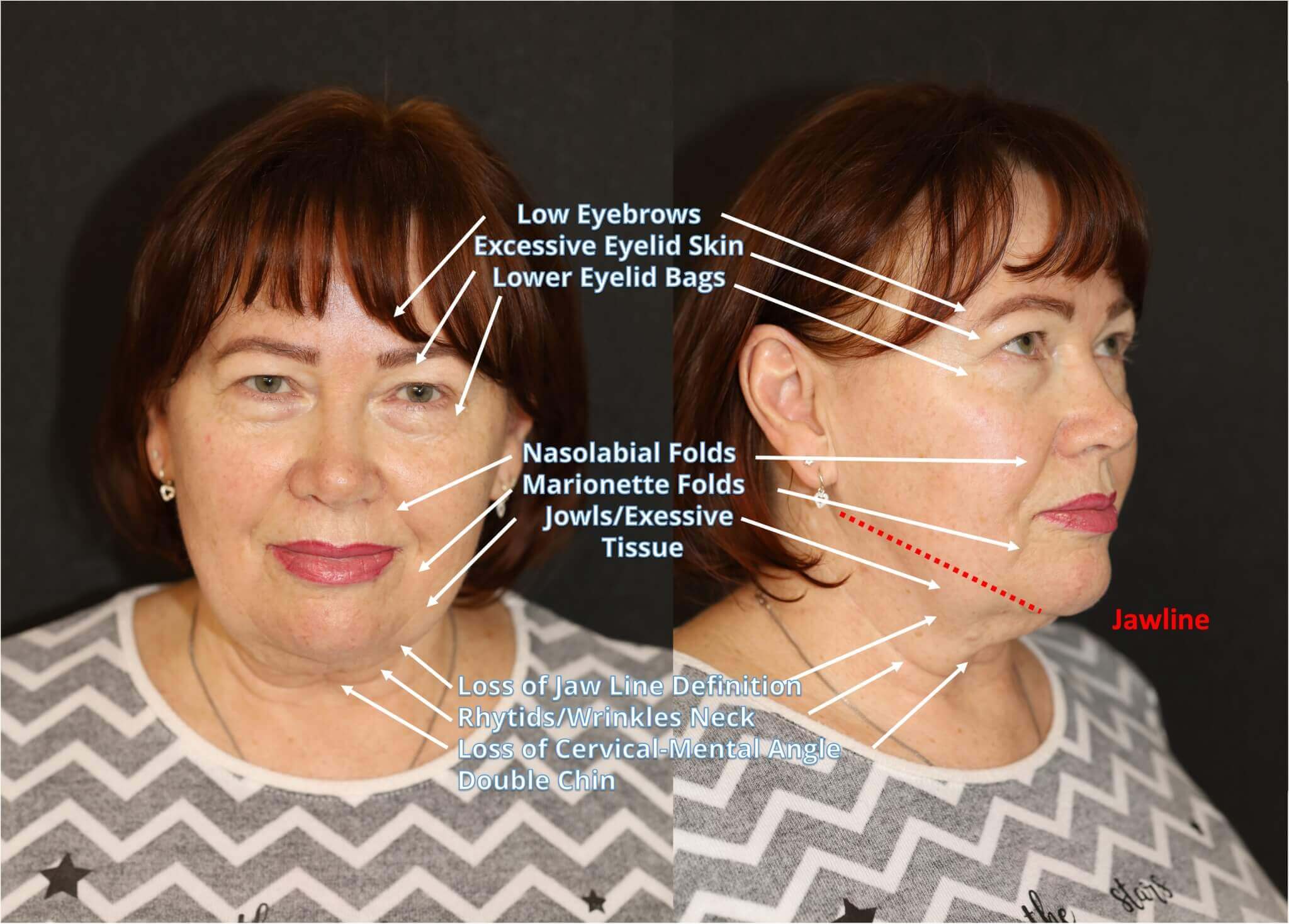
The following changes to the face develop with increasing age:
- Deepening of the laugh lines (nasolabial folds)
- Development of sagging cheeks (so-called “jowls”)
- Wrinkling at the corners of the mouth and to the sides
- Marionette wrinkles at the chin/cheek junction (mentolabial folds, mouth corner wrinkles)
- Loss of a clear lower jaw/chin line (“Jawline”, also jawline)
- Wrinkling as well as sagging, drooping skin and muscles in the neck area (platysma bands, platysma bands), so-called “turkey neck”
- Formation of a “double chin”
- Decreased chin-neck angle (cervico-mental angle)
- Changes in skin structure and skin quality
If several of the above-mentioned age-related changes are present, aesthetic facial surgery can help. As a particularly effective form of facial plastic surgery, rejuvenation by means of a deep plane facelift or extended deep plane facelift can be considered if facial rejuvenation is desired.
Injections with Botox (botulinum toxin), fillers and autologous fat are becoming increasingly popular, but there are clearly defined limits to their effect and effectiveness. In the case of forehead wrinkles, botulinum toxin can smooth and relax the muscles that cause these wrinkles. Volume can be added to the cheeks or lips and small wrinkles around the nose and mouth using fillers or autologous fat to restore youthfulness.
However, if there is excess, sagging skin that causes “sagging cheeks” and deeper wrinkles in the cheek/jaw area and also in the neck, neither Botox, fillers or autologous fat transplants (lipofilling) will be able to do much. This is because they cannot vertically reposition (“lift”) sagging, deeper tissue. This means that no tissue can be lifted using these minimally invasive procedures.
Anatomically correct repositioning of the affected tissue regions can only be achieved surgically through a facelift with an additional neck lift. The aim of the extended deep plane facelift is to make you look the way you are, only significantly younger. The character of your appearance from your younger years reappears instead of being lost. A rejuvenation of 10-15 years is possible without looking unnatural.
Rejuvenation is also the goal of fillers, but if the limits of injection techniques are disregarded, it can end up looking exaggerated and unnatural. Negative long-term effects have been described with excessive and incorrect application.
Although injectable fillers may appear to be a more cost-effective option than facelift surgery at first glance, they can end up being more expensive over a long period of time when calculating the total cost of maintaining a youthful appearance with fillers. A non-surgical facelift such as a thread lift, a liquid facelift, a vampire lift (autologous blood treatment with PRP therapy), skin treatment with so-called energy-based devices (e.g. laser therapy) and other non-surgical tightening techniques cannot replace a subtantial repositioning of the tissue layers by a professional facelift for effective rejuvenation by many years.
A deep plane facelift with neck lift performed by an experienced surgeon, on the other hand, achieves a highly effective but natural rejuvenation that lasts for decades.
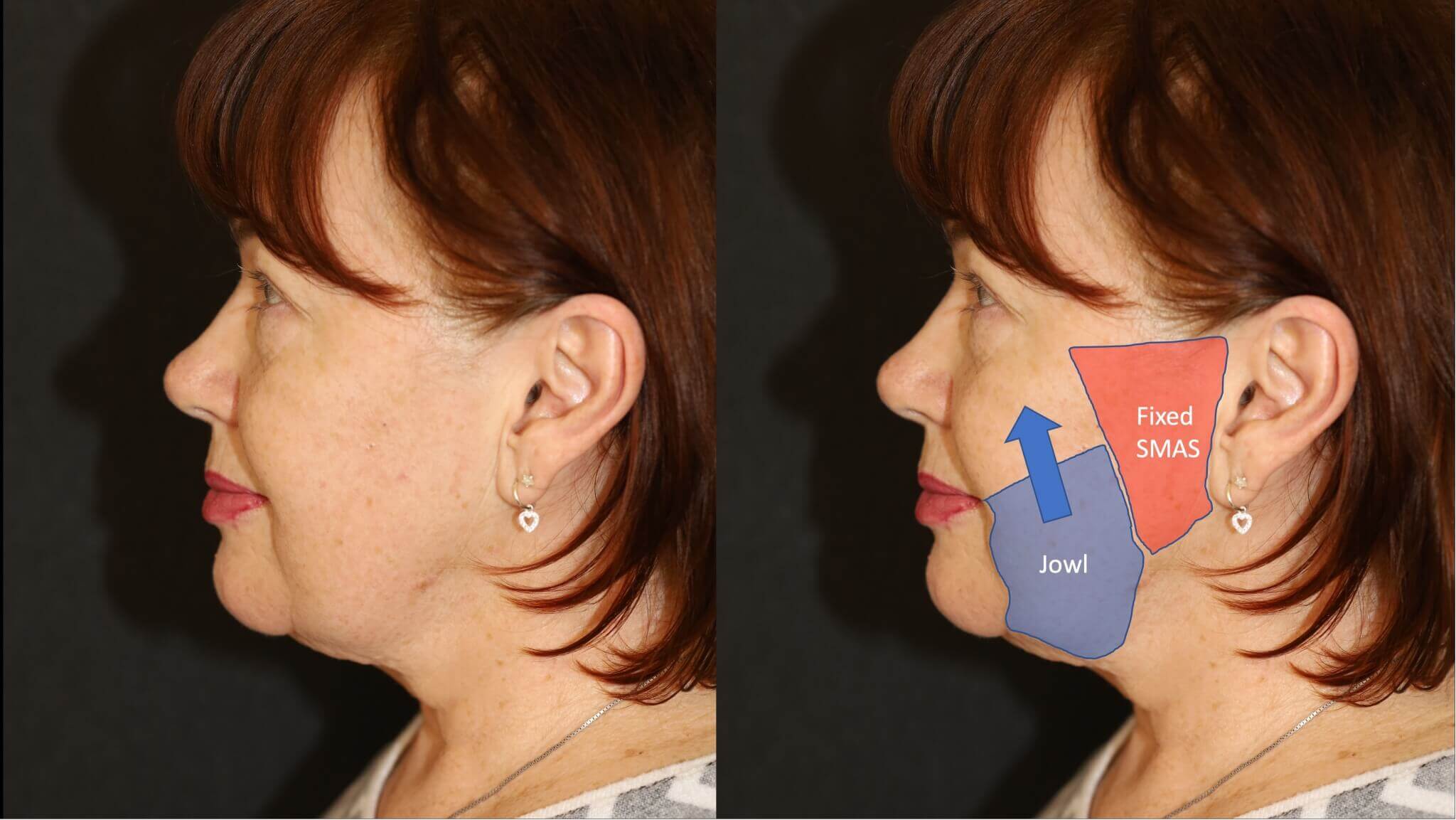
One of the deeper layers of the face is the SMAS (Superficial Muscular Aponeurotic System). While the lateral (side) parts of the face remain relatively fixed during the ageing process (“fixed SMAS”), the medial (middle) parts (“mobile SMAS”) continuously decrease with increasing age: this results in so-called sagging cheeks, which slide over the jaw and chin line to the neck area. The volume of the cheeks decreases and moves slightly forward towards the mouth. This results in a significant deepening of the laugh lines (nasolabial folds) not only when facial expressions are made, but also at rest. This can create a so-called “negative vector” in the corners of the mouth, i.e. the corners of the mouth tend to point downwards in the resting position, which can unintentionally lead to a rather unflattering sad and sometimes even grumpy facial expression. With a deep plane facelift, the age-related volume shifts in the face are largely reversed and the overlying skin tissue is loosely fitted in front of the ear without tension. With the deep plane facelift technique, the wrinkles on the neck are usually significantly improved by an accompanying neck lift.
Deep Plane Facelift - Advantages
Serious facelift methods have long since moved away from pure skin tightening (only removing small areas of skin in front of the ear) such as the subcutaneous facelift technique (minimally invasive facelift). Serious facelift techniques involve lifting and tightening the layer of connective tissue under the skin and still under the fatty tissue, the so-called SMAS (“superficial musculo-aponeurotic system”). Only then is the resulting excess skin in front of the ear removed and sutured without tension. The SMAS facelift (Superficial Muscular Aponeurotic System) has been described for this in the past. Different forms are the SMAS plication, sub-SMAS and high-SMAS facelift and other SMAS facelifts. The main differences between SMAS facelifts and the deep plane facelift are described below. However, to achieve a dramatic rejuvenation of the face in a natural way, SMAS tightening and skin resection alone are far from sufficient. A crucial question is in which area the SMAS layer is loosened and reattached. A distinction can be made between a lateral “fixed SMAS” in front of the ear and a “mobile SMAS” located more towards the center of the face.
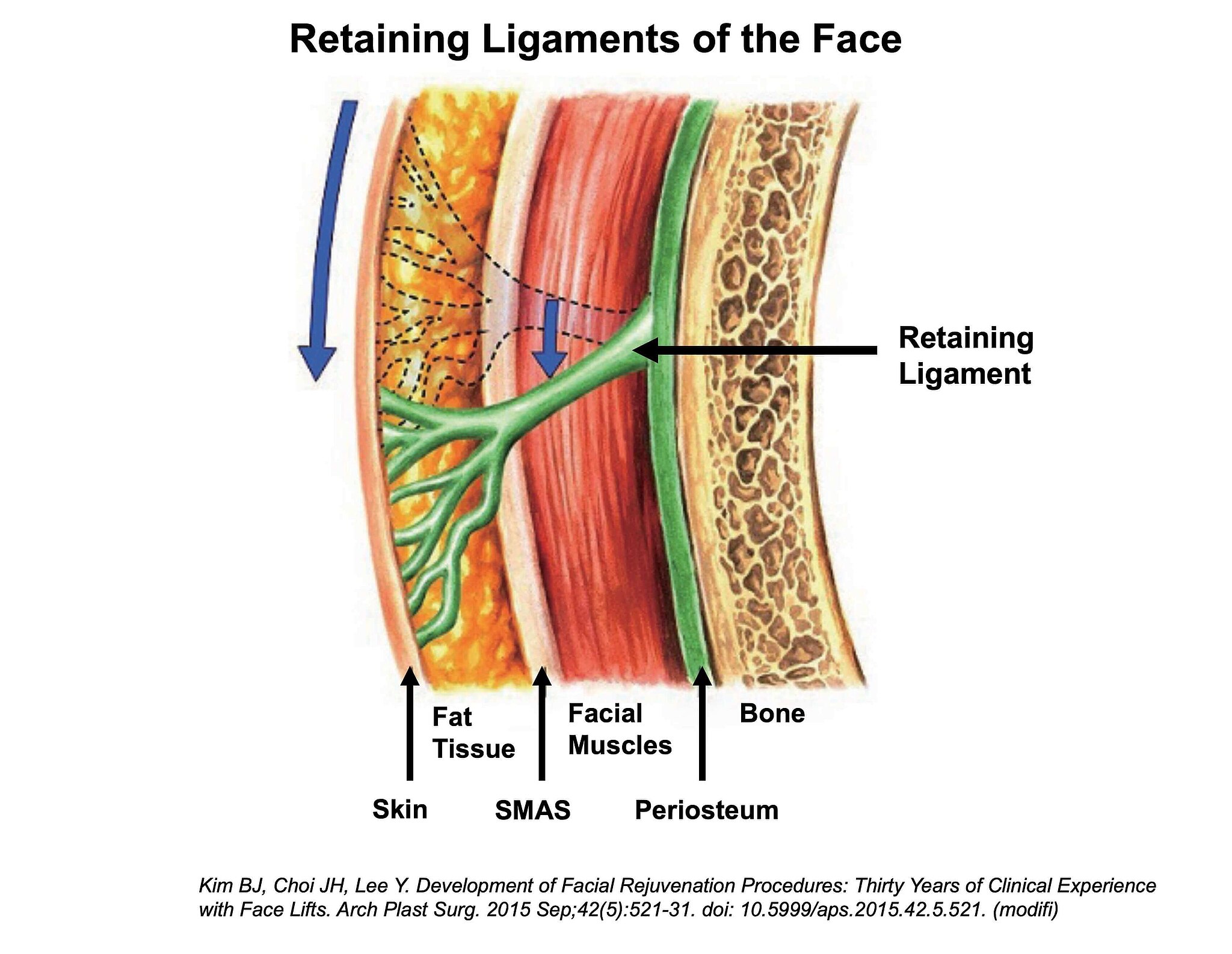
Furthermore, the various planar tissue and muscle layers of the face (in a parallel arrangement to the skin surface) are supported by a vertical retaining system. These so-called “retaining ligaments”, as we call them, which penetrate the parallel layers in different zones of the face almost orthogonally, act like supporting pillars and fix the parallel layers of tissue to bony prominences and other deeper tissues. If the tissue between these supporting structures becomes slack as we age, these supporting bands become visible on the surface of the skin as fixed wrinkles on the face. Although they also lengthen according to the law of gravity, the tissue between them becomes much deeper and begins to sag. This can be observed very clearly in the “sagging cheeks” above the lower jaw to the side of the corners of the mouth: while the chin and cheek tissue in front of and behind the sagging cheeks still appear quite well fixed, the tissue between them sags and extends downwards beyond the lower jaw to the neck area. This interrupts the jaw line, which makes the face appear much older. The wrinkles in front of it become much deeper and so-called marionette lines can form. The “fixed SMAS”, on the other hand, which is located in front of the ear, essentially remains in place even during the ageing process.

The Deep Plane Facelift can easily be combined with other facial rejuvenation methods:
- Brow lift / forehead lift / temple lift
- Endoscopic facelift technique
- Upper eyelid lift (blepharoplasty)
- Lower eyelid lift with relocation of the fatty tissue
- Canthopexy
- Lip lift (upper lip augmentation)
- Fat transfer (lipofilling with microfat and nanofat)
- Bichatectomy (slimming of the cheeks through targeted fat removal)
- Medical needling (Dermapen)
- Laser therapy for additional skin rejuvenation
- others
How does the Deep Plane Facelift work?
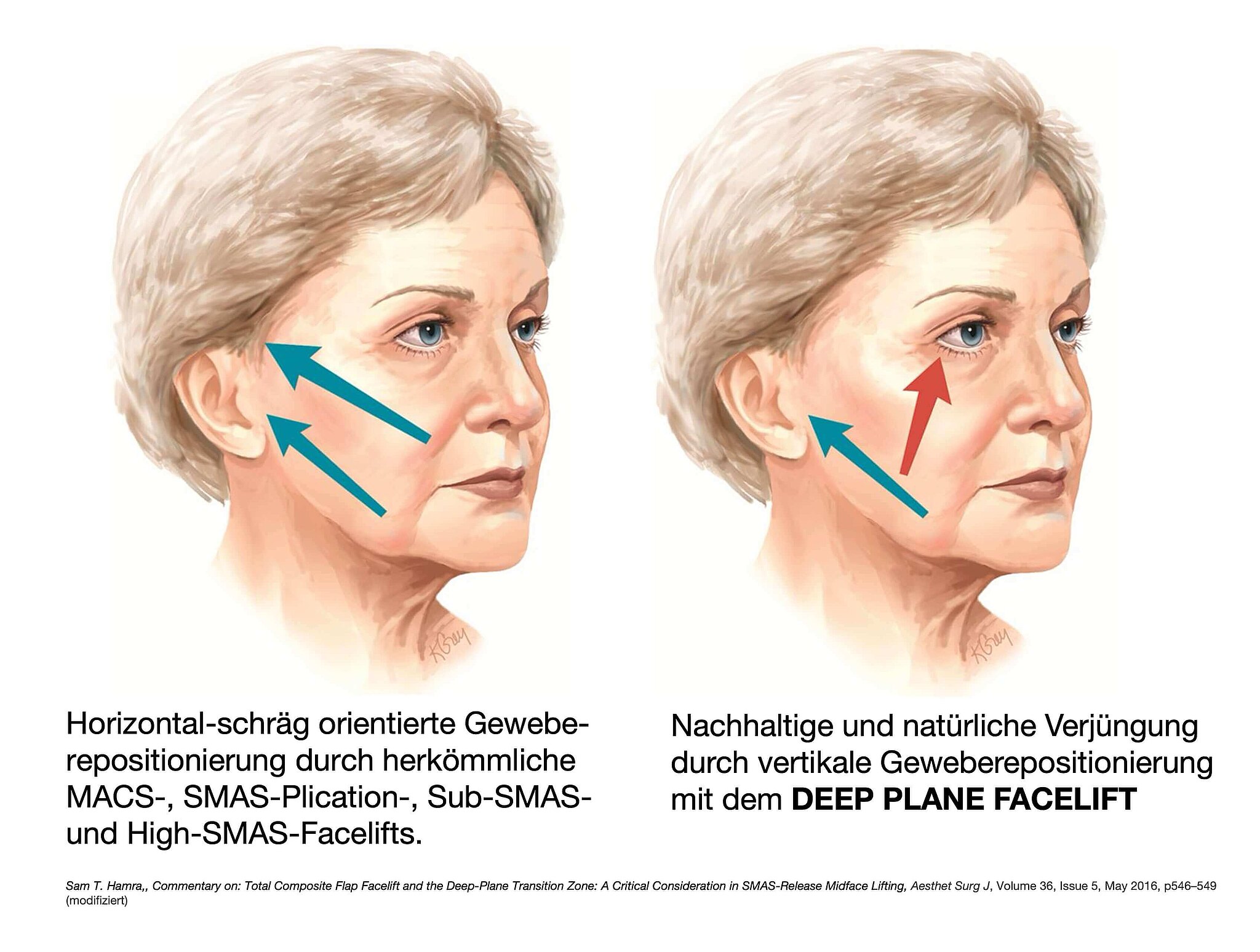
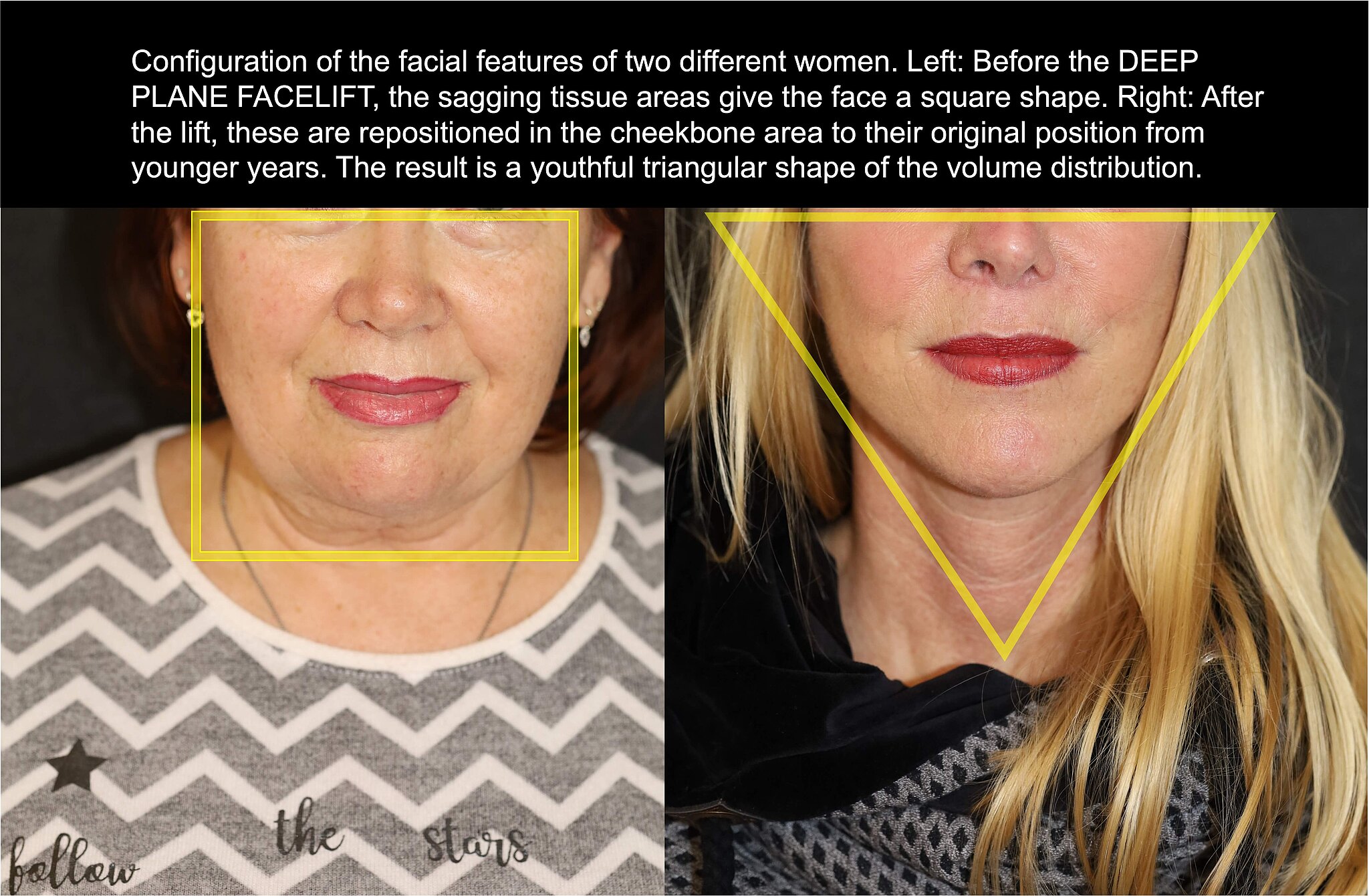
The upper midface region, which is reduced in volume with increasing age, is supplied with volume again by the lift and thus rejuvenated, as the middle and lower midface tissues are shifted back to their original juvenile position in the zygomatic bone and upper jaw region (malar region, prominent part above the zygomatic bone region). A “square facial shape” acquired with age is returned to a youthful “triangular shape” through volume displacement. This is made possible by an almost vertical resetting of the sagging tissue, which also takes into account the middle regions of the face in the area of the laugh lines (nasolabial folds), whereas other facelift techniques involve a much more horizontal and therefore less effective lift.
In contrast to other facelift methods, the neck region can be tightened significantly better with the extended deep plane facelift (DPFL) by consistently mobilizing the neck tissue. Natural-looking facelift results can be achieved with the DPFL. The effects of the facelift are long-lasting, patients still look much younger 10-15 years after the facelift as if they had not had it performed. Of course, a secondary DPFL can also be performed many years later.

As all the main retaining ligaments are released during the deep plane facelift, the face and especially the midface region can be repositioned significantly better and thus returned to its original position from the youthful years. Compared to other techniques, this is almost tension-free, as deeper facial layers (deep plane) are displaced. In particular, the skin is fitted in front of the ear with very little tension after appropriate reduction and adjustment. This results in very good and, above all, inconspicuous wound and scar healing. Tension and thus distortion of the tragus cartilage and earlobes can thus be consistently avoided. This means that only minimal scarring can be expected during a facelift, which remains hidden from the layman's eye. The recovery time after a facelift such as the deep plane facelift is comparable to other facelift techniques.
Facelifts are among the most complex procedures in aesthetic surgery. They require special expertise on the part of the surgeon that goes beyond the standard requirements of plastic surgery. Not everything that is offered as a facelift on the internet is actually a solid (and therefore effective) facelift that meets modern requirements and is based on current science and the latest anatomical findings. For patients, differentiating between the different levels of experience of different surgeons is actually very difficult to almost impossible in view of the wealth of available information, advertising, social media platforms and internet filter options. Nevertheless, and especially for this reason, the choice of your surgeon for a facelift should be made with particular care. Effective advertising terms such as “mini-lift” or “mini-lift” (minimally invasive facelift), “short-scar facelifts” and “weekend lift” usually have an attractive effect on interested patients, as they suggest that the desired goal of significant rejuvenation can be achieved with less invasive measures. In reality, however, they usually conceal the provider's lack of expertise in safely performing a deep and therefore effective facelift, such as the Deep Plane Facelift Germany in its most modern and consistent form.
Who is the best deep plane facelift surgeon? There is certainly no single best surgeon. Ideally, however, your surgeon will have specialized knowledge of facial anatomy and the facial nerve (facial nerve, facial nerve), which has been gained in their own anatomical studies on anatomical specimens (cadavers in anatomical institutes) and in hundreds of facial operations, especially in the field of reconstructive surgery and aesthetics alike. Individual weekend courses, video training (webinars) or even the study of ubiquitously available YouTube video clips are not sufficiently suitable for this. The generally observed trend towards non-invasive measures such as injection therapies using botulinum toxin (Botox), fillers and autologous fat as well as thread lifts etc., which only appear to be able to achieve consistent rejuvenation effortlessly in the blink of an eye, is also offset by a dwindling expertise in performing more invasive methods such as solid facelifts safely and consistently.

The higher the level of expertise and knowledge of the anatomical features of the face of your facelift surgeon, the more likely it is that in complex facial operations such as a facelift, the deeper layers (=deep plane) will be operated on, all the necessary in-depth steps for repositioning the tissue will be carried out and essential structures such as the facial nerve, which is essential for facial expression with its countless branches, will be safely protected in order to achieve optimal results. The concern of injuring the facial nerve and thus causing temporary or permanent paralysis of facial expressions is omnipresent among less trained surgeons and leads to tissues that are not mobilized consistently enough and thus to suboptimal results for facelift patients. Ask your surgeon specifically whether he/she actually mobilizes the tissues consistently, cutting all the essential retaining ligaments, right up to the nasolabial fold.
The author of this page fulfills the above criteria.
As part of his intensive research work on the facial nerve (facial nerve), he has consistently acquired the complex anatomy of the face in the dissection of over 100 halves of the face on cadavers in one of the largest series studied.He has also performed several hundred facial operations, some of which were very complex. Prof. Dr. med. Andreas Kehrer can look back on well over a thousand microsurgical procedures, some of them very complex, as well as several hundred microsurgical tissue transplants. This wealth of experience as a microsurgeon enables him, for example, to transplant small free functional muscles into the face with the necessary routine and a high degree of safety. The risk of suffering facial paralysis as a result of the deep plane facelift is therefore reduced to an absolute minimum.In his hands, the deep plane facelift is considered a very safe facelift procedure. His deep plane facelifts are performed under magnification using 4x magnifying glasses and the in-depth knowledge of the branches of the facial nerve (n. facialis) to be spared that he has acquired in research and microsurgery.
He regularly travels to Beverly Hills/Los Angeles, USA, in order to learn about the latest modifications and improvements to the technique in a personal exchange with the best facelift surgeons and to bring the latest trends in aesthetic facial surgery with him. With him, you really do get a genuine extended deep plane facelift with mobilization of the tissue up to the nasolabial fold. Deep Plane Facelift Before After pictures can be discussed together in a personal consultation.
In a large international study of high quality, a so-called meta-analysis, by the deep plane facelift specialist Jacono AA. et al., the risk of suffering temporary (i.e. non-persistent) damage to the facial nerve during a deep plane facelift was calculated to be 0.69% (n=1597).1
Literature:
1Jacono AA, Alemii AS, Russell JL. A meta-analysis of complication rates among different SMAS facelift techniques. Aesthetic Surg J 39:927-942, 2019
Excerpt from anatomical studies Prof. Dr. med. Andreas Kehrer::
[1] Kehrer A, Engelmann S, Bauer R, Geis S, Kehrer M, Prantl L, Bleys RLAW, Mandlik V. Anatomical study of the zygomatic and buccal branches of the facial nerve: application to facial reanimation procedures. Clin Anatom 2019
[2] Kehrer A, Engelmann S, Bauer R, et al. The nerve supply of zygomaticus major: Variability and distinguishing zygomatic from buccal facial nerve branches. Clin Anat 2018
[3] Kehrer A, Engelmann S, Ruewe M, Geis S, Taeger C, Kehrer M, Tamm ER, Bleys RLAW, Prantl L, Mandlik V. Perfusion maintains functional potential of denervated mimic muscles in early persistent facial paralysis which requires early microsurgical treatment - the histoanatomic basis of the extratemporal facial nerve trunk assessing axonal load in the context of possible nerve transfers. Clin Hemorheol Microcirc. 2018;70(1):1-13. doi: 10.3233/CH-189905.
[4] Mandlik V, Ruewe M, Engelmann S, Kehrer A et al. Significance of the Marginal Mandibular Branch in Relation to Facial Palsy Reconstruction - Assessment of Micro- and Macroanatomy including Axonal Load in 96 Facial Halves. Annals of Plastic Surgery 2019
[5] Engelmann S, Ruewe M, Geis S, Taeger CD, Kehrer M, Tamm ER, Bleys RLAW, Zeman F, Prantl L, Kehrer A. Rapid and Precise Semi-Automatic Axon Quantification in Human Peripheral Nerves. Sci Rep. 2020
[6] Sommerauer L, Engelmann S, Ruewe M, Anker A, Prantl L, Kehrer A. Effects of electrostimulation therapy in facial nerve palsy. Arch Plast Surg. 2020
[7] Ruewe M, Engelmann S, Huang CW, Klein SM, Anker AM, Lamby P, Bleys RLAW, Tamm ER, Prantl L, Kehrer A. Microanatomy of the Frontal Branch of the Facial Nerve: The Role of Nerve Caliber and Axonal Capacity, Plast Reconstr Surg. 2021

Many people interested in a facelift ask themselves: How much does a deep plane facelift cost? The deep plane facelift technique, which involves lifting the skin, fatty tissue and muscles (SMAS) together as a single unit and requires a great deal of experience, is currently performed by less than 5% of facelift surgeons, as it is a technically demanding procedure. However, in a practiced hand, the results of the deep plane facelift are significantly more rejuvenating and at the same time more natural than other techniques and last longer.
The cost of a facelift can depend on many variables, such as the extent and duration of the procedure, the degree of difficulty, the expertise of the surgeon and the type of anesthesia required. Prof. Dr. Andreas Kehrer adapts facelifts to each patient and their individual characteristics. He is also regarded by patients as a facelift specialist in Munich and offers the Deep Plane Facelift Munich.
Procedures such as the deep plane facelift are more complex than other forms of facelift. A deep plane facelift is therefore somewhat more expensive than other techniques, but also leads to significantly more natural results and reverses the signs of age in the middle and lower third of the face by an average of 10-15 years (depending on the initial age).
Do you have further questions, would you like to see the results or would you like to arrange a non-binding consultation?
Plastic facial surgery www.Prof-Kehrer.com
Prof. Dr. med. Andreas Kehrer /IN-Aesthetik
Further information and examples of complex surgical reconstructions for facial paralysis can be found at
www.fazialis.com
Publications Prof. Dr. med. Andreas Kehrer